






Price: Starting at $499 (Scales with Gift Card Add-on selection)
Duration: 12 Months of Online Access
Deliverables: 100 Hours of AAPA Category 1 CME Credit (PANRE Review Course), 300+ Practice Questions, Targeted Medical Content
Selecting the right continuing medical education (CME) package is a significant decision for any healthcare professional, particularly physician assistants facing the high-stakes PANRE or PANCE. While many providers offer incentives, the "best" choice is defined by the quality of the clinical content and the accreditation that actually counts toward your license renewal.
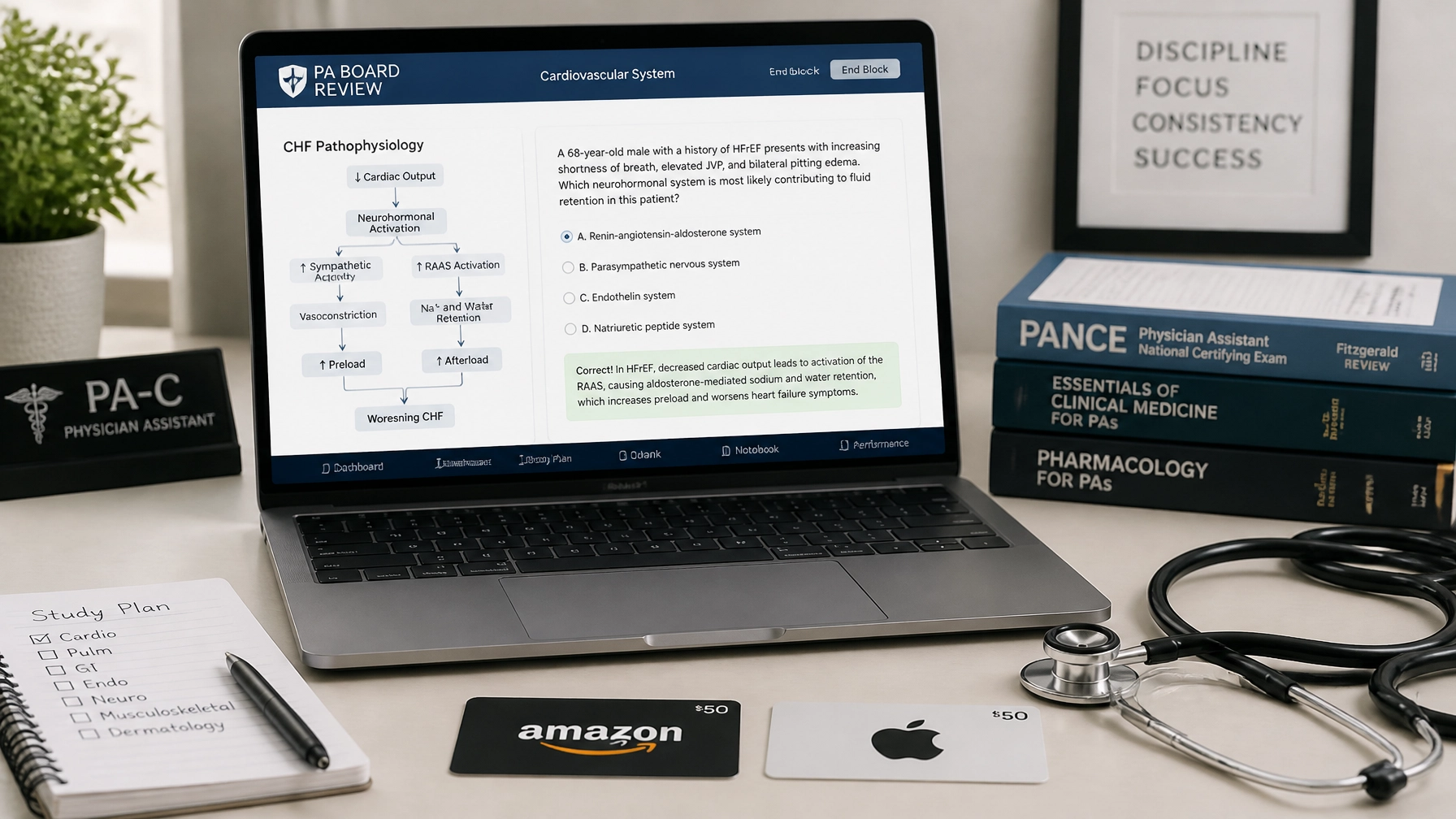
At CME Review Courses, we specialize in providing an efficient way to utilize your professional development funds. Our PANRE review course is specifically designed by physician assistants for physician assistants. When you choose a cme with gift card option, you are selecting a premium educational product with the ability to add on an Amazon or Apple Gift Card.
Comparing CME Gift Card Options
When comparing providers like CME4Life, Modern MedEd, or Audio Digest, you must look beyond the incentive. Many generic CME providers offer AMA PRA Category 1 Credits, which are excellent for physicians. However, for PAs, AAPA Category 1 Credit is the gold standard for NCCPA certification and state licensure requirements.
Our pance prep courses and PANRE materials offer up to 100 hours of AAPA Category 1 Credit. This is a critical distinction; while nurse practitioners and physicians find immense value in our content, PAs benefit from credits that are purpose-built for their professional requirements.
It is important to understand that the Amazon and Apple Gift Card add-ons (ranging from $100 to $1,500) are integrated into the total purchase price. These are NOT free gifts. They are educational add-ons designed to allow you to purchase further resources, such as medical textbooks, hardware, or software, to further enrich your clinical practice.

Efficient Internal Medicine and Hospitalist Review
For clinicians working in Internal Medicine or as Hospitalists, staying current on infectious disease management and cardiovascular guidelines is essential. Our content covers high-yield topics including Emergency Medicine, Family Medicine, and Orthopedics, ensuring that your study time translates directly to better patient outcomes.
Clinical Case Study: Internal Medicine
Your patient is a 68-year-old male presenting with a 3-day history of productive cough, pleuritic chest pain, and increased shortness of breath. He has a history of COPD and hypertension.
Vital Signs:
- BP: 112/74 mmHg
- HR: 102 bpm
- Temp: 101.8°F (38.8°C)
- SaO2: 91% on room air
- RR: 24 breaths/min
Physical examination reveals crackles at the right lung base and dullness to percussion. A chest X-ray confirms a right lower lobe infiltrate. You decide to admit him for community-acquired pneumonia (CAP).
Practice Question 1
What is the most appropriate initial empiric antibiotic regimen for this patient, given his comorbidities and need for hospitalization?
A) Levofloxacin monotherapy
B) Amoxicillin monotherapy
C) Ceftriaxone plus Azithromycin
D) Vancomycin plus Piperacillin-Tazobactam
Explanation:
The correct answer is C) Ceftriaxone plus Azithromycin. According to the ATS/IDSA guidelines for hospitalized patients with non-severe CAP, the preferred empiric treatment is a combination of a beta-lactam (like Ceftriaxone) and a macrolide (like Azithromycin), or a respiratory fluoroquinolone.
- A) Levofloxacin is a respiratory fluoroquinolone and could be used, but combination therapy is often preferred in patients with comorbidities like COPD to provide broader coverage.
- B) Amoxicillin is insufficient for a hospitalized patient with comorbidities.
- D) Vancomycin and Zosyn are reserved for patients with risk factors for MRSA or Pseudomonas, which are not suggested by this patient's initial presentation.
Practice Question 2
Three days into his hospitalization, the patient develops sudden onset confusion and a decrease in urine output to <0.5 mL/kg/hr. His HR increases to 120 bpm and BP drops to 88/54 mmHg. What is the most immediate next step in management?
A) Start intravenous vasopressors
B) Administer a 30 mL/kg isotonic crystalloid bolus
C) Perform an emergent CT Pulmonary Angiogram
D) Obtain a stat Echocardiogram
Explanation:
The correct answer is B) Administer a 30 mL/kg isotonic crystalloid bolus. This patient is showing signs of septic shock (hypotension, tachycardia, end-organ dysfunction/confusion). The first-line treatment for sepsis-induced hypotension is rapid fluid resuscitation with at least 30 mL/kg of IV crystalloid.
- A) Vasopressors are only initiated if the patient remains hypotensive after adequate fluid resuscitation (mean arterial pressure < 65 mmHg).
- C) and D) are diagnostic tests that may be necessary later, but they do not address the immediate hemodynamic instability.

Why Choose CME Review Courses for Your PANRE?
Navigating the NCCPA requirements can be daunting. We focus our curriculum on the high-yield areas you need to know for the exam. Our PANRE review course provides the 100 Category 1 AAPA credit hours you need in one comprehensive package.
Benefits of our CME Packages:
- PA-led instruction: Content is written by PAs who have successfully navigated the same exams you face.
- Broad Specialty Coverage: From Dermatology and Psychiatry to OB/GYN and Cardiology.
- Flexible Funding Utilization: Use your employer-provided CME money to its fullest potential by choosing the gift card add-on level that fits your remaining budget.
- Practice-Ready Questions: Our question banks mirror the clinical reasoning required for both the PANRE and daily practice.
Nurse practitioners also find significant value in our courses. While AAPA credit acceptance varies by state for NPs, many find the clinical depth of our Pharmacology course and specialty reviews far superior to generic offerings.

Maximizing Your Education with Gift Card Add-ons
As you evaluate different cme gift cards, consider what you need to be successful. Do you need a new iPad for referencing UpToDate at the bedside? An Amazon gift card add-on can facilitate that. Do you need to update your medical library with the latest surgical or emergency medicine texts? The add-on covers that too.
Our process is simple:
- Select your desired course (e.g., PANRE Review or Pharmacology).
- Choose your Gift Card add-on amount ($100 – $1,500).
- Complete your purchase and receive access to high-quality educational content and your selected gift card.
Remember, the priority is always the education. The gift card is a tool to support your continued learning journey.

Final Thoughts on Professional Development
Investing in a panre review course shouldn't be a chore. It should be a strategic move to secure your certification while improving your clinical acumen. By choosing a package that combines 100 hours of AAPA Category 1 credit with the flexibility of an Amazon or Apple gift card add-on, you are setting yourself up for success both in the exam room and at the patient's bedside.
Explore our full range of courses today and see why thousands of PAs, NPs, and physicians trust CME Review Courses for their professional training. And if you're looking for an app-based companion with 11,000+ questions for the PANCE, PACKRAT, and all 7 EOR rotations, check out PAtopia at cmereviewcourses.com/patopia-new-student-section/.